This page may contains affiliate links, which means the website may earn a small commission at no extra cost to you if you make a purchase through them. The HerHealth101 team only recommends products that align with our mission to support women’s health, and is not a reflection of any specific author. Your support helps keep this site growing. Thank you!
The decision to undergo a hysterectomy is often a major turning point in a woman’s health journey, and it is one that usually comes after a long road of managing symptoms that have affected her daily life. It is a common procedure that can be performed several different ways, and in my practice, I find that there can be a lot of confusion stemming from the terminology itself. So let’s discuss exactly what anatomical part each term refers to, and what is removed in each procedure, so you can understand exactly what is being proposed for your body and why.
Defining the Terminology
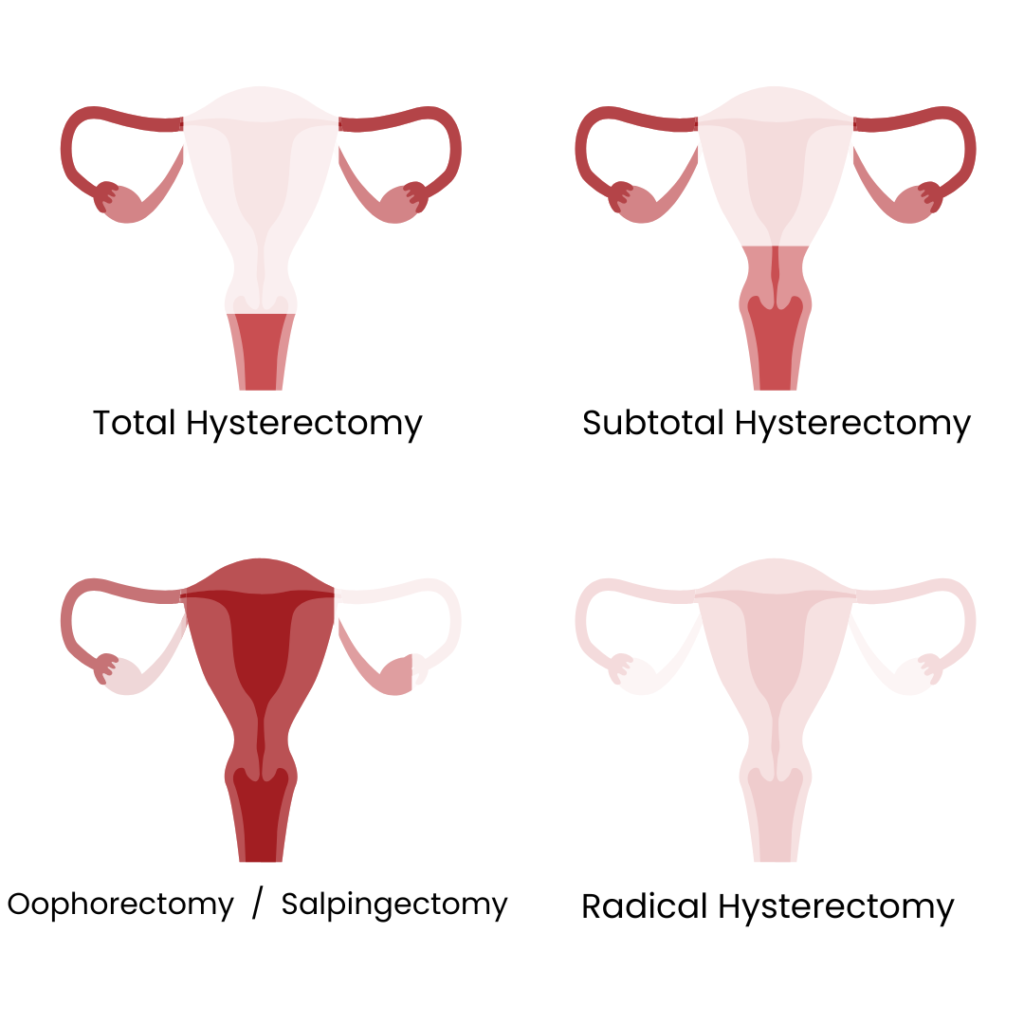
Then we move into the layers of what happens with the surrounding structures, specifically the fallopian tubes and ovaries. A salpingectomy is the removal of the fallopian tubes, and today, we often recommend this even if the ovaries are staying, as we’ve learned that many “ovarian” cancers actually begin in the tubes. An oophorectomy is the surgical removal of the ovaries. Since there are two fallopian tubes and ovaries, when both are taken, we add the word bilateral. If only one side is removed, we use the term unilateral.
The decision to remove only one ovary is often determined after a discussion about your specific condition, but it can be considered a “middle ground” because that single remaining ovary is usually more than capable of producing all the estrogen and progesterone your body needs, allowing you to avoid an immediate surgical menopause while still addressing an issue like a large cyst or endometriosis on the other side.
And finally, if everything is removed, including the uterus, cervix, both ovaries and fallopian tubes, the procedure may be referred to as a total hysterectomy with bilateral salpingo-oopherectomy, or in more extensive cases where part of the vagina and surrounding lymph nodes are also removed, a radical hysterectomy.

How a Surgeon Performs Hysterectomies
The technique the surgeon uses to perform the surgery is another vital piece of the puzzle. While an abdominal hysterectomy, the traditional “open” surgery, is sometimes necessary for very large fibroids or certain cancers, many surgeons are increasingly moving toward minimally invasive options. This includes vaginal hysterectomies, where the surgery is performed entirely through the vaginal canal with no external incisions, or laparoscopic and robotic-assisted methods that use tiny incisions in the abdomen. These newer techniques generally offer a much faster recovery, less post-operative pain, and a quicker return to normal activities. In terms of scarring, the minimally invasive techniques will be minimal with a few small (~1 cm) incisions in different areas of the abdomen. The abdominal open approach may be a larger scar several inches longs, however, in certain cases, this can be performed low along the bikini line (similar to the location of a cesarean section) and effectively hidden.

Recovery After a Hysterectomy
In the immediate days after your surgery, the focus is really on gentle movement and listening to your body. You will likely feel a sense of fatigue and some localized discomfort, but the priority is getting you up and walking early to help prevent blood clots and get your digestive system moving again. The main limitations you’ll most likely be instructed is to avoid heavy lifting or anything that increases your abdominal pressure, and nothing in the vagina for at least 6 weeks or until you’ve fully recovered.
Long-term, the most significant consideration often revolves around your hormones. If your ovaries were removed and you hadn’t yet reached menopause, you will experience surgical menopause almost immediately, which can bring on symptoms like hot flashes or vaginal dryness. This is a conversation you will have with your doctor well before the surgery so there is a plan in place for hormone replacement therapy or other supportive measures if they are right for you.

Knowing these differences empowers you to be an active participant in your care. Your reproductive health isn’t a one-size-fits-all situation, and the specific type of procedure chosen is a highly personalized decision based on your unique anatomy and your long-term health goals. By understanding the nuances of these surgeries, you can ensure that your path toward healing feels both informed and deeply respected.
About the Author:

Dr. Kai Dallas is a board certified and fellowship trained urogynecologist and pelvic reconstructive surgeon. He specializes in female pelvic health with clinical expertise in pelvic pain, pelvic organ prolapse and bladder disorders.